How CDC manipulated data to create ‘pandemic of the unvaxxed’ narrative
08/18/2021 / By News Editors
STORY AT-A-GLANCE
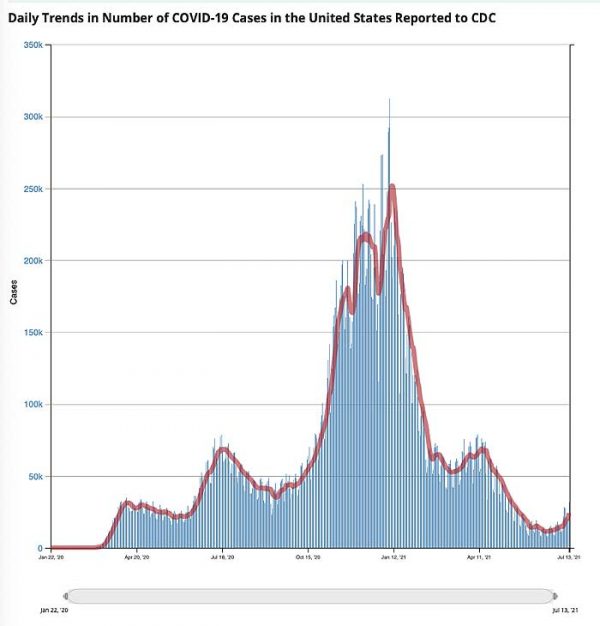
- According to Centers for Disease Control and Prevention data, COVID-19 “cases” have trended downward since peaking during the first and second week of January 2021. At first glance, this decline appears to be occurring in tandem with the rollout of COVID shots. However, “cases” were on the decline before a meaningful number of people had been vaccinated
- COVID-19 “cases” peaked January 8, 2021, when more than 300,000 new positive test results were recorded on a daily basis. By February 21, that had declined to a daily new case count of 55,000
- COVID-19 gene modification injections were granted emergency use authorization at the end of December 2020, and by February 21, only 5.9% of American adults had been fully injected with two doses. Despite such a low injection rate, new “cases” had declined by 82%
- The best explanation for a declining COVID-19 case rate appears to be natural immunity from previous infections. A study by the National Institutes of Health suggests COVID-19 prevalence was 4.8 times higher than previously thought, thanks to undiagnosed infection
- The survivability of COVID-19 outside of nursing homes is 99.74%. If you’re under the age of 40, your chance of surviving a bout of COVID-19 is 99.99%. You can’t really improve your chances of surviving beyond that, so COVID shots cannot realistically end the pandemic
(Article by Dr. Joseph Mercola republished from Articles.Mercola.com)
According to Centers for Disease Control and Prevention data,1 COVID-19 “cases” have trended downward since peaking during the first and second week of January 2021.
At first glance, this decline appears to be occurring in tandem with the rollout of COVID shots. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot. By mid-April, an estimated 31% had received one or more shots,2 and as of July 13, 48.3% were fully “vaccinated.”3
However, as noted in a July 12, 2021, STAT News article,4 “cases” had started their downward trend before COVID shots were widely used. “Following patterns from previous pandemics, the precipitous decline in new cases of Covid-19 started well before a meaningful number of people had been vaccinated,” Robert M. Kaplan, Professor Emeritus at the UCLA Fielding School of Public Health, writes. He continues:
“Nearly 50 years ago, medical sociologists John and Sonja McKinlay examined5 death rates from 10 serious diseases: tuberculosis, scarlet fever, influenzae, pneumonia, diphtheria, whooping cough, measles, smallpox, typhoid, and polio. In each case, the new therapy or vaccine credited with overcoming it was introduced well after the disease was in decline.
More recently, historian Thomas McKeown noted6 that deaths from bronchitis, pneumonia, and influenza had begun rapidly falling 35 years before the introduction of new medicines that were credited with their conquest. These historical analyses are relevant to the current pandemic.”
‘Case’ Decline Preceded Widespread Implementation of Jab
As noted by Kaplan, COVID-19 “cases” peaked in early January 2021. January 8, more than 300,000 new positive test results were recorded on a daily basis. By February 21, that had declined to a daily new case count of 55,000. COVID-19 gene modification injections were granted emergency use authorization at the end of December 2020, but by February 21, only 5.9% of American adults had been fully vaccinated with two doses.
Despite such a low vaccination rate, new “cases” had declined by 82%. Considering health authorities claim we need 70% of Americans vaccinated in order to achieve herd immunity and stop the spread of this virus, this simply makes no sense. Clearly, the COVID shots had nothing to do with the decline in positive test results.
To be clear, reported cases mean positive test results, and we now know the vast majority of positive PCR tests have been, and still are, false positives. They’re not sick. They simply had a false “positive.” Right now, we’re also faced with yet another situation that complicates attempts at data analysis, and Kaplan understandably did not address any of these confounding factors.
But just so you’re aware, if you have been fully “vaccinated,” then the CDC recommends running the PCR test at a cycle threshold (CT) of 28 or lower, which dramatically lowers your chance of a false positive result, but if you are unvaccinated, the PCR test is recommended to be run at a CT of 40 or higher, virtually guaranteeing a false positive.
This is just one way by which the CDC is manipulating data to make the COVID shots appear more effective than they are. This also allows them to falsely claim that the vast majority of new cases are among the unvaccinated.
Naturally, if unvaccinated are tested in such a way as to maximize false positives, then they’re going to make up the bulk of the so-called caseload. In reality, though, the vast majority of them aren’t sick.
Meanwhile, those who have received the jabs only count as a COVID case if they’re hospitalized and/or die with a positive test result. These widely differing testing strategies skew the data and allow for false interpretations to be made.
Natural Immunity Explains Decline in Cases
As noted by Kaplan, the most reasonable explanation for declining rates of SARS-CoV-2 appears to be natural immunity from previous infections, which vary considerably from state to state.7 He goes on to cite a study8 by the National Institutes of Health, which suggests SARS-CoV-2 prevalence was 4.8 times higher than previously thought, thanks to undiagnosed infection.
In other words, they claim that for every reported positive test result, there were likely nearly five additional people who had the infection but didn’t get a diagnosis. To analyze this data further, Kaplan calculated the natural immunity rate by dividing the new estimated number of people naturally infected by the population of any given state. He writes:9
“By mid-February 2021, an estimated 150 million people in the U.S. (30 million times five) may have had been infected with SARS-CoV-2. By April, I estimated the natural immunity rate to be above 55% in 10 states: Arizona, Iowa, Nebraska, North Dakota, Oklahoma, Rhode Island, South Dakota, Tennessee, Utah, and Wisconsin.
At the other end of the continuum, I estimated the natural immunity rate to be below 35% in the District of Columbia, Hawaii, Maine, Maryland, New Hampshire, Oregon, Puerto Rico, Vermont, Virginia, and Washington …
By the end of 2020, new infections were already rapidly declining in nearly all of the 10 states where the majority may have had natural immunity, well before more than a minuscule percentage of Americans were fully vaccinated. In 80% of these states, the day when new cases were at their peak occurred before vaccines were available.
In contrast, the 10 states with lower rates of previous infections were much more likely to experience new upticks in Covid-19 cases in March and April … By the end of May, states with fewer new infections had significantly lower vaccination rates than states with more new infections.”
COVID Shots Cannot Eliminate COVID-19
So, SARS-CoV-2 cases were actually higher in states where natural immunity was low but vaccination rates were high. Meanwhile, in states where natural immunity due to undiagnosed exposure was high, but vaccination rates were low, the daily new caseload was also lower.
This makes sense if natural immunity is highly effective (which, historically it has always been and there’s no reason to suspect SARS-CoV-2 is any different in that regard). It also makes sense if the COVID shots aren’t really offering any significant protection against infection, which we also know is the case.
Vaccine manufacturers have already admitted these COVID shots will not provide immunity, meaning they will not prevent you from being infected. The idea behind these gene modification injections is that if/when you do get infected, you’ll hopefully experience milder symptoms, even though you’re still infectious and can spread the virus to others.
Kaplan ends his analysis by saying that COVID shots are a safer way to achieve herd immunity, and that they are “the best tool available for assuring that the smoldering fire of [COVID-19] is extinguished.” I disagree, based on two major issues.
First, and perhaps most importantly, this is an untested “vaccine” and we have no idea of the short-term let alone long-term damage it will cause, as any reasonable effort at collecting this data has been actively suppressed. Secondly, the survivability of COVID-19 outside of nursing homes is 99.74%. If you’re under the age of 40, your chance of surviving a bout of COVID-19 is 99.99%.10,11,12
You can’t really improve your chances of surviving beyond that, so COVID shots cannot realistically end the pandemic. Meanwhile, the COVID shots come with an ever-growing list of potential side effects that can take years if not decades off your natural life span. The shots are particularly unnecessary for anyone with natural immunity,13 yet that’s what the CDC recommends.14
Why Push COVID Jab on Those with Natural Immunity?
In January 2021, Dr. Hooman Noorchashm, a cardiac surgeon and patient advocate, sent a public letter15 to the U.S. Food and Drug Administration commissioner detailing the risks of vaccinating individuals who have previously been infected with SARS-CoV-2, or who have an active SARS-CoV-2 infection.
He urged the FDA to require prescreening for SARS-CoV-2 viral proteins to reduce the risk of injuries and deaths following vaccination, as the vaccine may trigger an adverse immune response in those who have already been infected with the virus. In March 2021, Fox TV host Tucker Carlson interviewed him about these risks. In that interview, Noorchashm said:16
“I think it’s a dramatic error on part of public health officials to try to put this vaccine into a one-size-fits-all paradigm … We’re going to take this problem we have with the COVID-19 pandemic, where a half-percent of the population is susceptible to dying, and compound it by causing totally avoidable harm by vaccinating people who are already infected …
The signal is deafening, the people who are having complications or adverse events are the people who have recently or are currently or previously infected [with COVID]. I don’t think we can ignore this.”
In an email to The Defender, Noorchashm fleshed out his concerns, saying:17
“Viral antigens persist in the tissues of the naturally infected for months. When the vaccine is used too early after a natural infection, or worse during an active infection, the vaccine force activates a powerful immune response that attacks the tissues where the natural viral antigens are persisting. This, I suggest, is the cause of the high level of adverse events and, likely deaths, we are seeing in the recently infected following vaccination.”
Despite being widely ignored, Noorchashm continues to push for the implementation of prevaccine screening using PCR or rapid antigen testing to determine whether the individual has an active infection, and an IgG antibody test to determine past infection.
If either test is positive, he recommends delaying vaccination for a minimum of three to six months to allow your IgG levels to wane. At that point, he recommends testing your blood IgG level and use that as a guide to decide the timing of your vaccination.
Those with Natural Immunity Have Higher Risk of Side Effects
Mere weeks after Noorchashm’s letter to the FDA, an international survey18 confirmed his concerns. After surveying 2,002 people who had received a first dose of COVID-19 vaccine, they found that those who had previously had COVID-19 experienced “significantly increased incidence and severity” of side effects, compared to those who did not have natural immunity.
The mRNA COVID-19 vaccines were linked to a higher incidence of side effects compared to the viral vector-based COVID-19 vaccines, but tended to be milder, local reactions. Systemic reactions, such as anaphylaxis, flu-like illness and breathlessness, were more likely to occur with the viral vector COVID-19 vaccines.
Like Noorchashm before them, the researchers called on health officials to reevaluate their vaccination recommendations for people who’ve had COVID-19:19
“People with prior COVID-19 exposure were largely excluded from the vaccine trials and, as a result, the safety and reactogenicity of the vaccines in this population have not been previously fully evaluated. For the first time, this study demonstrates a significant association between prior COVID19 infection and a significantly higher incidence and severity of self-reported side effects after vaccination for COVID-19.
Consistently, compared to the first dose of the vaccine, we found an increased incidence and severity of self-reported side effects after the second dose, when recipients had been previously exposed to viral antigen.
In view of the rapidly accumulating data demonstrating that COVID-19 survivors generally have adequate natural immunity for at least 6 months, it may be appropriate to re-evaluate the recommendation for immediate vaccination of this group.”
CDC Misrepresents Data to Push Jab on Those with Immunity
So far, the CDC has refused to change its stance on the matter. Instead, officials at the agency seem to have doubled down and actually go out of their way to misrepresent data in an effort to harass those with natural immunity to inappropriately take the jab, which is clearly clinically unnecessary.
In a report issued by the CDC’s Advisory Committee on Immunization Practices (ACIP) December 18, 2020, the Pfizer-BioNTech COVID-19 vaccine was said to have “consistent high efficacy” of 92% or more among people with evidence of previous SARS-CoV-2 infection.20
After looking at the Pfizer trial data, Rep. Thomas Massie — a Republican Congressman for Kentucky and an award-winning scientist in his own right — discovered that’s completely wrong. In a January 30, 2021, Full Measure report, investigative journalist Sharyl Attkisson described how Massie tried, in vain, to get the CDC to correct its error. According to Massie:21,22
“There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either …
It [the CDC report] says the exact opposite of what the data says. They’re giving people the impression that this vaccine will save your life, or save you from suffering, even if you’ve already had the virus and recovered, which has not been demonstrated in either the Pfizer or the Moderna trial.”
After multiple phone calls, CDC deputy director Dr. Anne Schuchat finally acknowledged the error and told Massie it would be fixed. “As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it,” Schuchat said in the recorded call.
January 29, 2021, the CDC issued its supposed correction, but rather than fix the error, they simply rephrased the mistake in a different way. This was the “correction” they issued:
“Consistent high efficacy (?92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
As you can see, the “correction” still misleadingly suggests that vaccination is effective for those previously infected, even though the data showed no such thing. Children of ever-younger ages are also being pushed to get the COVID jab, even though they have the absolute lowest risk of dying from COVID-19 of any group.
Data23 from the first 12 months of the pandemic in the U.K. show just 25 people under the age of 18 died from or with COVID-19.24 In all, 251 children under 18 were admitted to intensive care between March 2020 and February 2021. The absolute risk of death from COVID-19 in children is 2 in 1 million.
Vaccine Provides Far Less Protection Than Natural Immunity
While some claim vaccine-induced immunity offers greater protection against SARS-CoV-2 infection than natural immunity, historical and current real-world data simply fail to support this non-common sense assertion.
As recently reported by Attkisson25,26 and David Rosenberg 7 Israeli National News,27 recent Israeli data show those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection.
Among the 7,700 new COVID cases diagnosed so far during the current wave of infections that began in May 2021, 39% were vaccinated (about 3,000 cases), 1% (72 patients) had recovered from a previous SARS-CoV-2 infection and 60% were neither vaccinated nor previously infected. Israeli National News notes:28
“With a total of 835,792 Israelis known to have recovered from the virus, the 72 instances of reinfection amount to 0.0086% of people who were already infected with COVID.
By contrast, Israelis who were vaccinated were 6.72 times more likely to get infected after the shot than after natural infection, with over 3,000 of the 5,193,499, or 0.0578%, of Israelis who were vaccinated getting infected in the latest wave.”
Breakthrough Infections Are on the Rise
Other Israeli data also suggest the limited protection offered by the COVID shot is rapidly eroding. August 1, 2021, director of Israel’s Public Health Services, Dr. Sharon Alroy-Preis, announced half of all COVID-19 infections were among the fully vaccinated.29 Signs of more serious disease among fully vaccinated are also emerging, she said, particularly in those over the age of 60.
Even worse, August 5, Dr. Kobi Haviv, director of the Herzog Hospital in Jerusalem, appeared on Channel 13 News, reporting that 95% of severely ill COVID-19 patients are fully vaccinated, and that they make up 85% to 90% of COVID-related hospitalizations overall.30
Other areas where a clear majority of residents have been vaccinated are also seeing spikes in breakthrough cases. In Gibraltar, which has a 99% COVID jab compliance rate, COVID cases have risen by 2,500% since June 1, 2021.31
US Outbreak Shatters ‘Pandemic of Unvaccinated’ Narrative
An investigation by the CDC32,33 also dispels the narrative that we’re in a “pandemic of the unvaccinated.” An outbreak in Barnstable County, Massachusetts, resulted in 469 new COVID cases among residents who had traveled into town between July 3 and July 17, 2021.
Of these cases, 74% were fully vaccinated, as were 80% of those requiring hospitalization.Most, but not all, had the Delta variant of the virus. The CDC also found that fully vaccinated individuals who contract the infection had as high a viral load in their nasal passages as unvaccinated individuals who got infected.34 This means the vaccinated are just as infectious as the unvaccinated. According to Attkisson:35
“CDC’s newest findings on so-called ‘breakthrough’ infections in vaccinated people are mirrored by other data releases. Illinois health officials recently announced36 more than 160 fully-vaccinated people have died of Covid-19, and at least 644 been hospitalized; 10 deaths and 51 hospitalizations counted in the prior week …
In July, New Jersey reported 49 fully vaccinated residents had died of Covid; 27 in Louisiana; 80 in Massachusetts … Nationally, as of July 12, CDC said it was aware of more than 4,400 people who got Covid-19 after being fully vaccinated and had to be hospitalized; and 1,063 fully vaccinated people who died of Covid.”
It is important to note this data is over 1 month old now and it is likely that many thousands of fully “vaccinated” have now died from COVID-19.
Natural Immunity Appears Robust and Long-Lasting
An argument we’re starting to hear more of now is that even though natural immunity after recovery from infection appears to be quite good, “we don’t know how long it’ll last.” This is rather disingenuous, seeing how natural immunity is typically lifelong, and studies have shown natural immunity against SARS-CoV-2 is at bare minimum longer lasting than vaccine-induced immunity.
Here’s a sampling of scholarly publications that have investigated natural immunity as it pertains to SARS-CoV-2 infection. There are several more in addition to these:37
| Science Immunology October 202038 found that “RBD-targeted antibodies are excellent markers of previous and recent infection, that differential isotype measurements can help distinguish between recent and older infections, and that IgG responses persist over the first few months after infection and are highly correlated with neutralizing antibodies.” |
| The BMJ January 202139 concluded that “Of 11,?000 health care workers who had proved evidence of infection during the first wave of the pandemic in the U.K. between March and April 2020, none had symptomatic reinfection in the second wave of the virus between October and November 2020.” |
| Science February 202140 reported that “Substantial immune memory is generated after COVID-19, involving all four major types of immune memory [antibodies, memory B cells, memory CD8+ T cells, and memory CD4+ T cells]. About 95% of subjects retained immune memory at ~6 months after infection. Circulating antibody titers were not predictive of T cell memory.
Thus, simple serological tests for SARS-CoV-2 antibodies do not reflect the richness and durability of immune memory to SARS-CoV-2.” A 2,800-person study found no symptomatic reinfections over a ~118-day window, and a 1,246-person study observed no symptomatic reinfections over 6 months. |
| A February 2021 study posted on the prepublication server medRxiv41 concluded that “Natural infection appears to elicit strong protection against reinfection with an efficacy ~95% for at least seven months.” |
| An April 2021 study posted on medRxiv42 reported “the overall estimated level of protection from prior SARS-CoV-2 infection for documented infection is 94.8%; hospitalization 94.1%; and severe illness 96·4%. Our results question the need to vaccinate previously-infected individuals.” |
| Another April 2021 study posted on the preprint server BioRxiv43 concluded that “following a typical case of mild COVID-19, SARS-CoV-2-specific CD8+ T cells not only persist but continuously differentiate in a coordinated fashion well into convalescence, into a state characteristic of long-lived, self-renewing memory.” |
| A May 2020 report in the journal Immunity44 confirmed that SARS-CoV-2-specific neutralizing antibodies are detected in COVID-19 convalescent subjects, as well as cellular immune responses. Here, they found that neutralizing antibody titers do correlate with the number of virus-specific T cells. |
| A May 2021 Nature article45 found SARS-CoV-2 infection induces long-lived bone marrow plasma cells, which are a crucial source of protective antibodies. Even after mild infection, anti-SARS-CoV-2 spike protein antibodies were detectable beyond 11 months’ post-infection. |
| A May 2021 study in E Clinical Medicine46 found “antibody detection is possible for almost a year post-natural infection of COVID-19.” According to the authors, “Based on current evidence, we hypothesize that antibodies to both S and N-proteins after natural infection may persist for longer than previously thought, thereby providing evidence of sustainability that may influence post-pandemic planning.” |
| Cure-Hub data47 confirm that while COVID shots can generate higher antibody levels than natural infection, this does not mean vaccine-induced immunity is more protective. Importantly, natural immunity confers much wider protection as your body recognizes all five proteins of the virus and not just one. With the COVID shot, your body only recognizes one of these proteins, the spike protein. |
| A June 2021 Nature article48 points out that “Wang et al. show that, between 6 and 12 months after infection, the concentration of neutralizing antibodies remains unchanged. That the acute immune reaction extends even beyond six months is suggested by the authors’ analysis of SARS-CoV-2-specific memory B cells in the blood of the convalescent individuals over the course of the year.
These memory B cells continuously enhance the reactivity of their SARS-CoV-2-specific antibodies through a process known as somatic hypermutation. The good news is that the evidence thus far predicts that infection with SARS-CoV-2 induces long-term immunity in most individuals.” |
| Another June Nature paper concluded that “In the absence of vaccination antibody reactivity [to the receptor binding domain (RBD) of SARS-CoV-2], neutralizing activity and the number of RBD-specific memory B cells remain relatively stable from 6 to 12 months.” According to the authors, the data suggest “immunity in convalescent individuals will be very long lasting.” |
What Makes Natural Immunity Superior?
The reason natural immunity is superior to vaccine-induced immunity is because viruses contain five different proteins. The COVID shot induces antibodies against just one of those proteins, the spike protein, and no T cell immunity. When you’re infected with the whole virus, you develop antibodies against all parts of the virus, plus memory T cells.
This also means natural immunity offers better protection against variants, as it recognizes several parts of the virus. If there are significant alternations to the spike protein, as with the Delta variant, vaccine-induced immunity can be evaded. Not so with natural immunity, as the other proteins are still recognized and attacked.
Not only that but the COVID jabs actually actively promote the production of variants for which they provide virtually no protection at all, while those with natural immunity do not cause variants and are nearly universally protected against them.
If we are to depend on vaccine-induced immunity, as public health officials are urging us to do, we’ll end up on a never-ending booster treadmill. Boosters will absolutely be necessary, as the shot offers such narrow protection against a single protein of the virus. Already, Moderna has publicly stated that the need for additional boosters is expected.49
Ultimately It’s About Wealth Transfer, Power and Control
Government agencies typically don’t issue recommendations without ulterior motives. Since current recommendations make absolutely no sense from a medical and scientific standpoint, what might the reason be for these illogical and reprehensibly unethical recommendations to inject people who don’t need it with experimental gene modification technology?
Why are they so hell-bent on getting a needle in every arm? And why are they refusing to perform any kind of risk-benefit analysis?
Data already indicate these COVID-19 injections could be the most dangerous medical product we’ve ever seen, and a June 24, 2021, peer-reviewed study published in the medical journal Vaccines warned we are in fact killing nearly as many with the shots as would die from COVID-19 itself.50
Using data from a large Israeli field study and two European drug reactions databases, they recalculated the NNTV for Pfizer’s mRNA shot. To prevent one case of COVID-19, anywhere between 200 and 700 had to be injected. To prevent a single death, the NNTV was between 9,000 and 50,000, with 16,000 as a point estimate.
Meanwhile, the number of people reporting adverse reactions from the shots was 700 per 100,000 vaccinations. For serious side effects, there were 16 reports per 100,000 vaccinations, and the number of fatal side effects was 4.11 per 100,000 vaccinations.
The final calculation suggested that for every three COVID-19 deaths prevented, two died from the shots. “This lack of clear benefit should cause governments to rethink their vaccination policy,” the authors concluded.
As has become the trend, a letter expressing “concern” about the study was published June 28, 2021, resulting in the paper being abruptly retracted July 2, 2021, against the authors’ objections. They disagreed with the accusation that their data and subsequent conclusion were misrepresentative, but the paper was retracted before they had time to publish a rebuttal.
Based on everything we’ve discovered so far, it seems a pandemic virus industrial complex is running the show, with a goal to eliminate medical rights and personal freedoms in order to centralize power, control and wealth.
By the looks of things, the COVID-19 mass psychosis and loss of any rational thinking by nearly half the population will continue to persist as long as the propaganda continues. Fear will continue and if need be, other engineered viruses may be released, for which they’ll create even more gene modification injections.
If they get their way, we’ll be stuck on a vaccine treadmill that may radically reduce the population. One of the most obvious solutions that anyone can do is to just say no to these shots. At bare minimum, wait. I believe the truth will eventually be so overwhelming, it’ll sweep away the confusion and the lies.
Read more at: Articles.Mercola.com and Deception.news.
Tagged Under: big government, CDC, conspiracy, corruption, covid19, deception, health freedom, lies, Medical Tyranny, natural immunity, pandemic, propaganda, vaccine
RECENT NEWS & ARTICLES